6 Cystic Fibrosis
6.1 Line types
Peripheral catheters are typically geared for use for a few days and will then need replacement. They are rarely a first choice for a child requiring a CF tune-up.
“Mid-lines” - the Monash term for a venous catheter of about 12 cm length inserted into a peripheral vein. These lines terminate in veins of a bigger calibre and are less prone to cause obstruction or phlebitis than pure peripheral catheters.
They are often considered when we know we will require venous access for more than just a few days up to two weeks. While they can be inserted under vision only in an awake child on the ward, in reality many younger (and older!) patients will require at least some sedation and the use of ultrasound to guide placement.
PICCs - peripherally inserted central catheters. PICCs are the line of choice for children likely to require longer-term intravenous treatment. PICCs can typically remain in place for six weeks and in many children are appropriate remain in the home and even school environment. Because they are long and thin resistence can be an issue.[^11]
Which drugs are we likely to use and where is the child going to receive treatment?
Choice of venous access does not only depend on the duration of treatment but to a large degree on which treatment the child is going to receive and where the child is going to be treated.
Will we get by with peripheral venous access?
This might be an option in an older child with good veins who tolerates this procedure well. Or is this a younger child that suffers unduly with intravenous access? Speak to play-therapy as they can make a tremendous difference to how the child will experience the procedure.
If peripheral access does not seem a feasible option a PICC or “mid-line” inserted under GA with the help of anaesthetics might be the way to go.
Do we need any blood tests? Send a path slip detailing the tests and the right tubes with the child and make sure the anaesthetist knows about our request.
Organising line insertion of PICC and central lines by anaesthetics
PICC and conventional central lines placed via anaesthetics are requested via the following procedure:
❖
Call the anaesthetist in charge at MMC on x3051 to discuss your line plan and fasting instructions for the patient.
Once you’ve agreed on a plan with anaesthetics enter your request into EMR:
In the orders section type CVAD, then select ANAES Central Venous Access Device (CVAD) Insertion PAEDIATRIC
Complete all fields, including all details of the referral and a Request for Emergency Surgery. This is required to obtain access to an operating theatre. Only if your patient already has a procedure booked in theatre during which the line can be placed (for instance a bronchoscopy) and no additional theatre space is required can you omit the Request for Emergency Surgery.
Both a verbal as well as an EMR referral need to be done before anaesthetics will proceed to insertion of a line.
Please note that anaesthetics are unable to accept any referrals for above lines out of hours (ie after 5 pm Monday-Friday and during weekends or public holidays).
A child with cystic fibrosis will most frequently be admitted under the Respiratory bed card. If the admission is for a non-CF related issue, such as appendectomy, we will usually share a bed card with the primary admitting team. General anaesthesia and subsequent inability to adhere to the patient’s regular physiotherapy regimen can lead to significant deterioration. Advance planning of procedures in conjunction with the CF-team can often reduce procedure-related impairments in the child’s health.
The majority of CF-related admissions are semi-elective for a tune-up. Typical clinical scenarios leading to a tune-up include:
Significant deterioration in lung function
Eradication-therapy for Pseudomonas aeruginosa — now mostly done at home with TOBI (Tobramycin for inhalation) — or other significant pathogens (Burkholderia cepacia, Mycobacterium abscessus).
Persistent moist cough.
“Prophylactic” - before travelling overseas, exam periods, etc.
Frequently the child will have had treatment at home with oral and inhaled antibiotics before being admitted to hospital. If this is the child’s first hospital admission, make sure the family have received a copy of our brochure “What should you expect on your child’s first visit to hospital”. The CF-coordinator can supply you with copies. Give it a read yourself if you haven’t yet.
Admission logistics
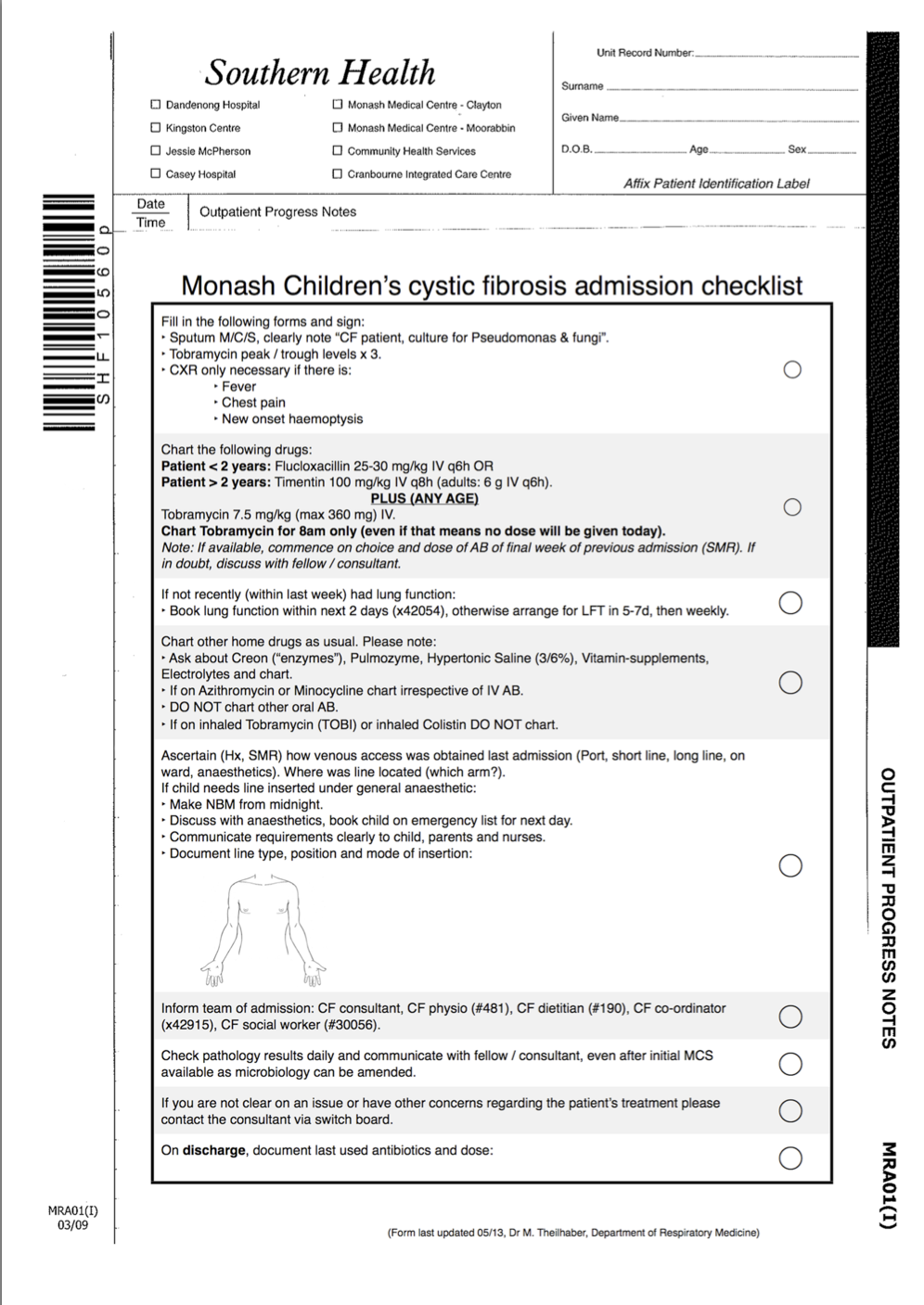
Print two documents off the Intranet:
Cystic Fibrosis Admission Checklist from http://cfadmit.notlong.com
myCF Inpatient Care Plan from http://is.gd/cfplan
Both links will open a PDF document that prints on a blank sheet of A4 paper on any hospital printer.
❖
The CF-checklist will guide you along the admission of a patient with CF. Tick the list off to ensure you’ve covered all areas and file it into the patient’s history. You still need to document the admission in the patient’s history in your usual concise way, outlining the reason for admission, current and past issues, your clinical examination findings and patient assessment and treatment plan.
CF “colours”
Avoiding airway colonisation with aggressive bacteria is a significant factor in achieving long-term health in CF. While none of these bacteria pose a risk to immunocompetent persons with normal airways, other people with CF can become colonised by contact to an affected patient. Immuno-suppressed patients may also be at risk.
To avoid cross-infection many CF-centres assigned patients to groups according to the type of bacterial airway-colonisation. We have also used this approach by assigning colour codes to groups of bacteria and segregated all clinics, lung-function appointments and gym-sessions based on these categories.
However, the rise of non-tuberculous mycobacteria as a new threat to the health of people with cystic fibrosis has led to a rethinking about cross-infection in the hospital. We’ll talk more about this in the next segment.
We have changed the way our clinics run, bringing them in line with international best practice. Upon arrival to clinic the patients enter their individually assigned clinic rooms and remain there for the duration of the appointment. This reduces the risk of cross-infection by confining the patient (and their potentially pathogenic airway bacteria) to a well supervised area. In addition, we use portable HEPA-devices in our clinic rooms that filter out >99.9% of all bacteria. Medical, allied health and social work staff rotate through the patient’s room rather than the patient going to see these providers. Lung function testing also occurs in the patient’s room using a calibrated portable device.
As the adult CF clinics still follow the colour system we continue assigning patients into colour groups based on their latest airway cultures. Once grouped into a specific (non-blue) pathogen cohort, return to the blue cohort (standard precautions) requires at least 6 month and 3 negative cultures. In case of a positive airway culture for M. abscessus a minimum of 12 months since positive culture and 4 airway cultures negative for M abscessus are required before return to the blue cohort can occur.
| Cohort Colour | Any sputum culture positive | Action |
| Blue | No Pseudomonas or NTM | Standard precautions |
| Green | Pseudomonas | Isolate from CF patients who do not have Pseudomonas |
| Yellow | Melbourne strain (M16) clonal Pseudomonas | Isolate from all M16 negative patients with CF, other chronic lung disease or immunocompromise |
| Purple | Burkholderia cepacia, MRSA or non-tuberculous mycobacteria (NTM) | Isolate from patients with CF, other chronic lung disease or immunocompromise, including those who are already in the purple cohort (many strains). |
❖
CF outpatient management
When we reviewed the overall clinical exposure junior medical staff had to CF care we found that the majority of contactd occured in inpatient care.
Inpatient care has traditionally been the area where paediatric JMS spend most of their working time and received the most clinical exposure. Paradoxically, it is also the area of clinical care where the majority of paediatricians spend the least amount of time. The majority of clinical contacts for paediatricians typically occurs in outpatient encounters - an area we found clinical JMS training to been lacking. To improve this imbalance we made significant changes to the training opportunities for the ATR.
The centrepiece of the redesigned training is the ATR’s participation in the weekly CF outpatient clinic. This opens up the range of CF outpatient care with its distinct challenges and rewards. The ATR has the opportunity to build long-term relationships with patients and families, monitor progress, and experience the significant benefits of multi-disciplinary CF care as an integral member of a long-term partnership between patients, families and the Monash CF-team.
The ATR acts as first port of call for outpatient queries and requests during business hours. This includes clinical scenarios such as deciding whether to commence an outpatient on antibiotics, reviewing and acting on pathology reports for outpatients and helping families who requesting scripts.
Queries from outpatients go through the CF-coordinators and they are usually able to sort out most of the questions. They will seek the ATR’s input when medical decision making is required. As with all clinical matters, please discuss or escalate to the on-call consultant if you are uncertain on how best to proceed.
Emerging pathogens
Cystic fibrosis is a dynamic field. Unfortunately, this is not only true for new therapies but also for emerging pathogens. Beginning in the early 1990s, centres around the world have seen a marked increase in the number of CF patients presenting with pulmonary infection with non-tuberculous mycobacteria (NTM). These bacteria pose a major challenge to those affected by CF and health services world-wide as they are extremely difficult to treat and can lead to severe, sometimes precipitous deterioration.
Two particular NTM organisms most commonly affect people with CF:
Mycobacterium avium complex (MAC): a group of closely related slow-growing mycobacteria. Well over 2/3 of NTM cultured from airway secretions of CF patients belong to this group. There have been no reports of patient to patient transmission.
Mycobacterium abscessus: a rapid growing mycobacterium. Patient to patient transmission has been reported.
Culturing NTM from a CF-patient’s airway does not equate to clinically relevant NTM-infection. NTM are ubiquitous and sporadic airway occurrence is to be expected. There is a wide clinical spectrum from those without any symptoms to those severely affected. Accordingly, a positive culture for NTM is only one piece of the puzzle. Of those with a first positive NTM-culture about 40% will go on to clinical NTM-disease requiring treatment.
Why not just treat at first signs of NTM?
Good question. It has a fairly straight forward, somewhat depressing answer: NTM are notoriously difficult to treat. Treatment is time-consuming, requires long-term complex iv therapy and severe side-effects often make the treatment very difficult to tolerate for patients. To add insult to injury chances of successfully eradicating M abscessus are very low (MAC are usually easier to treat). More often than not we think of suppressing NTM in this setting rather than eradicating.
So, if we’re deciding to embark on this treatment path we need to make sure the substantial burden of treatment does in fact outweigh the detrimental effects caused by the disease.
Differentiating between NTM-infection and NTM-disease
Research is occurring internationally to generate best practice guidelines to address the question on how best to select patients for treatment of NTM, which treatment combination to use and for how long to treat.
Keeping in mind that NTM-disease should present with significant clinical deterioration we look at the problem along 3 axis:
Microbiological evidence
- Positive NTM culture x2 (sputum) or x1 (BAL) over 12 month period
Clinical / radiological evidence
Unexplained loss in LFTs
Increased respiratory symptoms
Constitutional symptoms
Progression of radiographic features c/w NTM-infection
Absence of co-morbidities that could explain the patient’s clinical state (treat aggressively and re-evaluate)
Co-infections
Sputum clearance
Reactive airways disease
Nutritional deficits
Cystic Fibrosis Related Diabetes (CFRD)
ABPA (Allergic Bronchopulmonary Aspergillosis)
Sinus disease
Organising lung function tests
The majority of lung function tests you request will be for patients with CF. We usually check lung function in patients with CF when they come in for a tune-up and then monitor progress on a weekly basis. Your ATR or consultant will let you know if lung-function assessments are required at other times.
Because of the risk of cross infection between patients we have completely changed the way we see paediatric CF patients in clinic.
Make sure you understand the colour coding of CF-patients according to their colonisation with certain bacteria (see previous chapter). We work hard to avoid crossover of patients of different colours in the Respiratory Department. This applies even more so to the Lung Function Lab.
To book in your patient for lung function tests, call ext 42278 and let them know:
UR number, patient name and age
CF patient? If yes: which colour cohort does the patient belong to
Any other precautions the lab needs to be aware of (such as immuno-suppression)
Which tests you want and how urgent they are
Make sure you communicate any special requirements. If you require a physiotherapist to be present during a test (such as for a Mannitol trial), make sure both the lab and the physiotherapist know about it. Similarly, if you want Salbutamol given to test for reversibility of bronchoconstriction, say so.
Respiro - the pulmonary lab results database
All tests performed in our pulmonary lab are documented in the department’s database. The latest iteration of the software is called Respiro. Look out for the Respiro icon on your computer desktop:
If you can’t locate the icon you might not yet have access to this resource. Please speak to Paul Finlay in the lab who will organise access for you.
Once you’ve run Respiro, you need to login. Use ‘physician’ for both id and password and you will be greeted by Respiro’s main screen.
Click on ‘I’ on the left, then enter the name of the patient you’re looking for on the right. Make sure you separate last and first name by using a dash (‘-’) rather than a comma (‘,’).
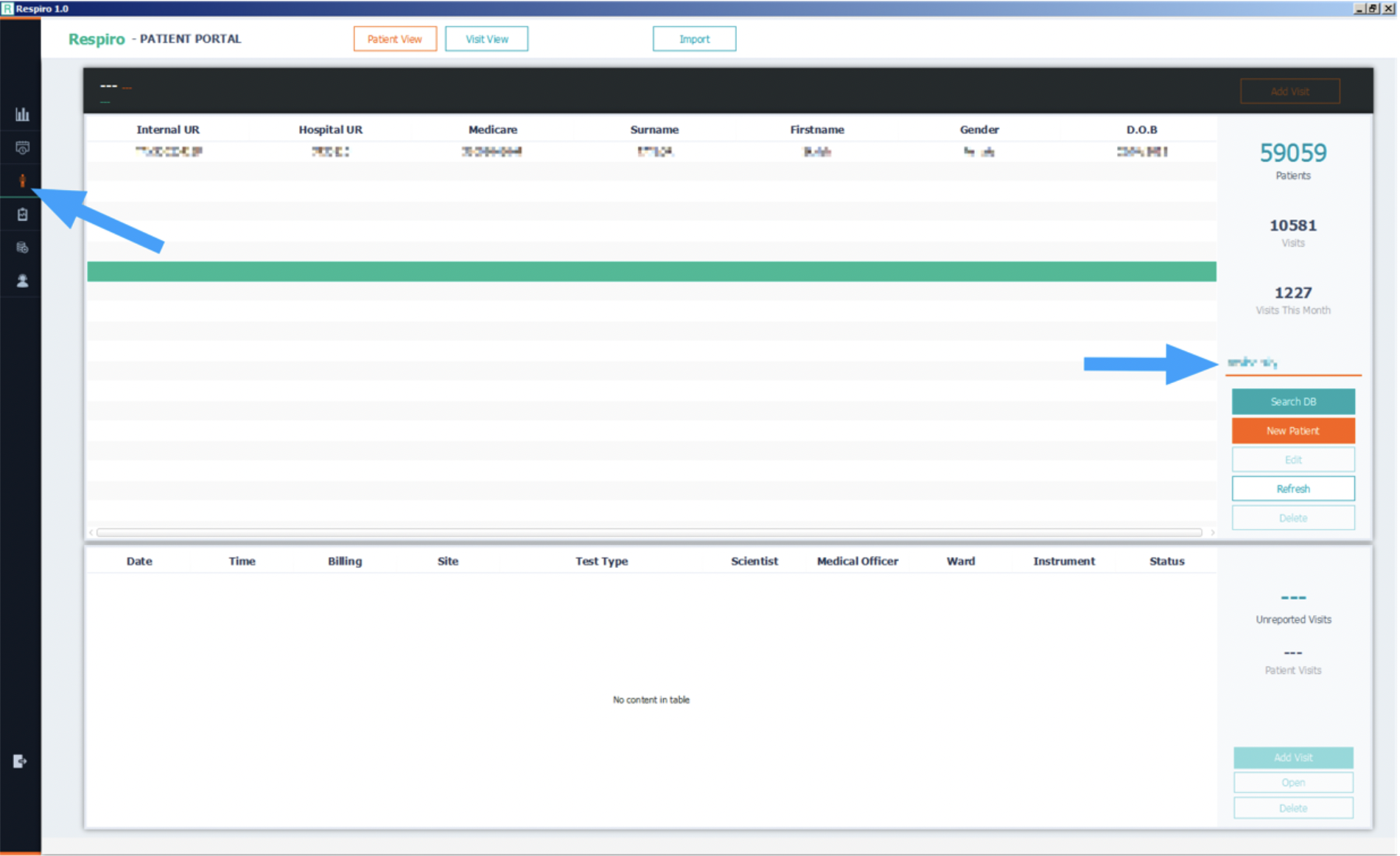
Click on ‘Search DB’ to find patients.
Patients fitting this name will be listed in the top table, their corresponding tests can be found in the bottom table.
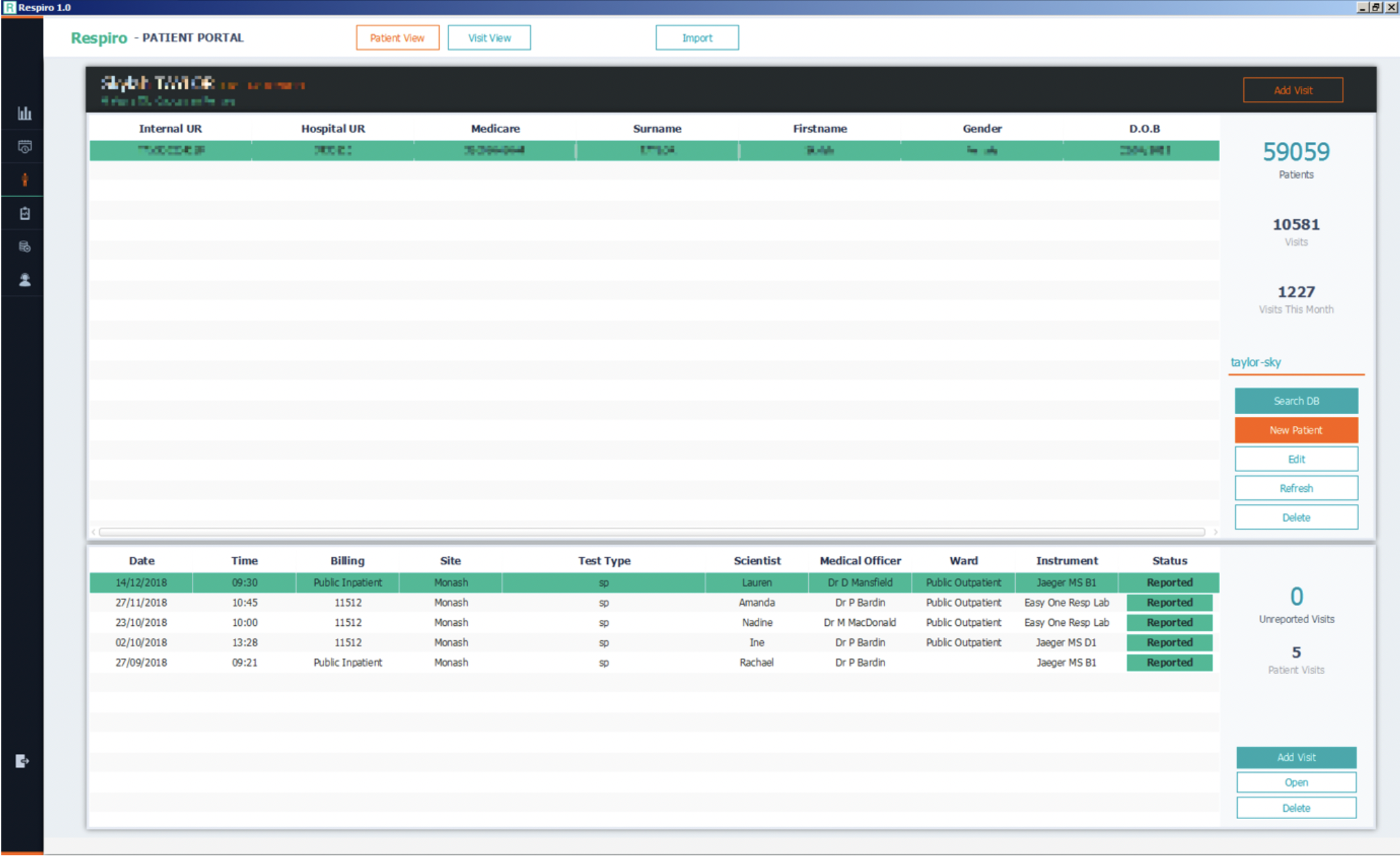
Double click a test entry to the results of that test.
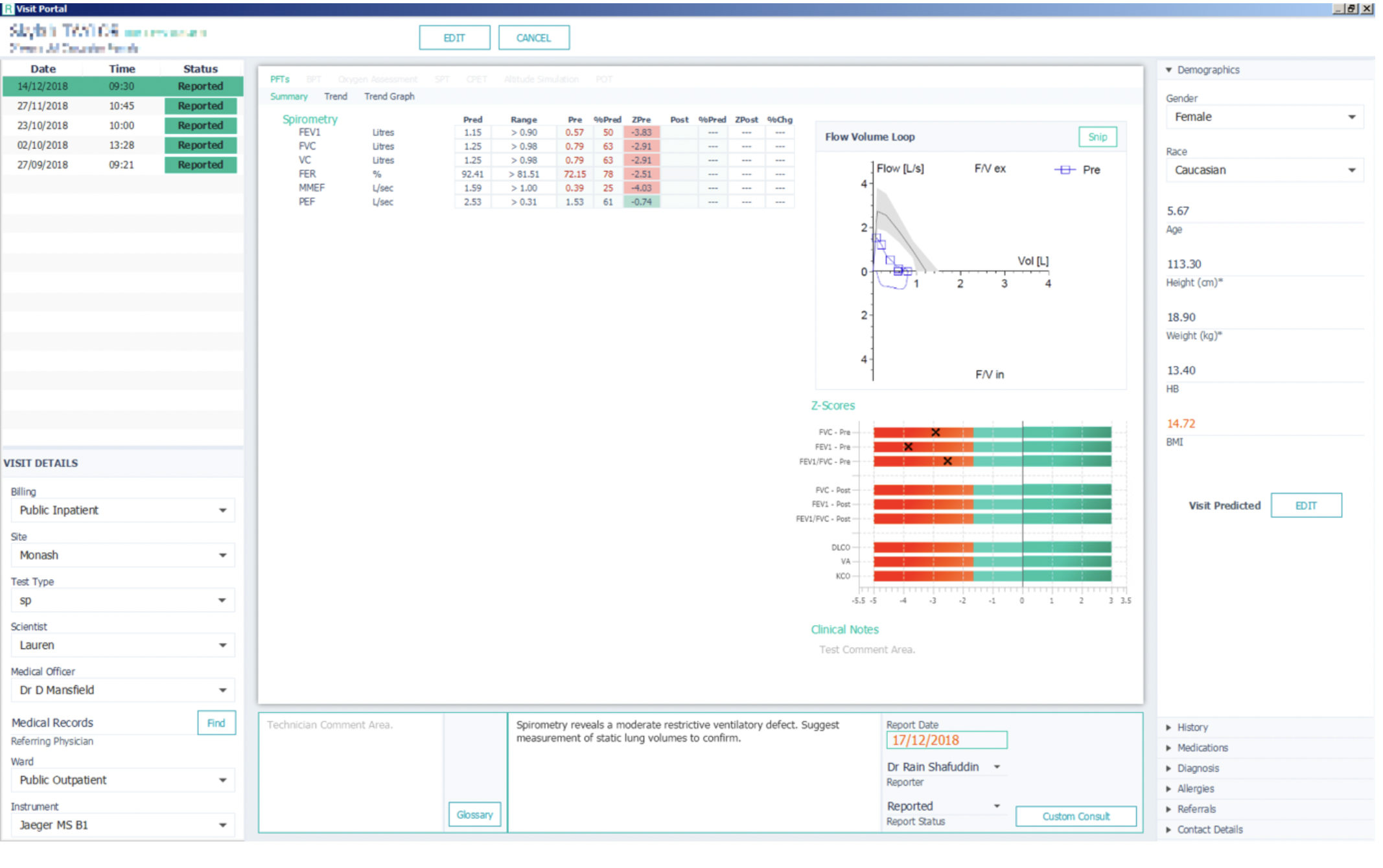
You can also plot trends over time. Click on ‘Trend Graph’ to chose the parameters you would like Respiro to plot for you.
Other functionality will be added to Respiro over time. Speak to the lab staff for particular functionality you may be interested in.
The CF team-meeting
CF is a complex multi-system disease that significantly affects the lives of patients, their care-givers and their social networks. Contemporary CF-care is embedded within multi-disciplinary teams which provides superior care over a single provider approach.
In any organisation, keeping up communication pathways becomes a challenge as the number of people involved increases. This topic has recently re-surfaced in other areas of medicine such as the renewed focus on medical handover of patients and the impact its quality has on subsequent patient care.
The main multi-disciplinary CF-meeting occurs weekly on Tuesday afternoons for 90 minutes, 45 minutes each are allocated for discussion of paediatric and adult patients. All CF-team members attend: medical (CF physicians, registrars and residents) and allied health (physiotherapy, dietetics, social work, nursing, CF-coordinator).
The objective of the meeting is to inform all team-members on patient progress, identify patients who require a more intense focus and establish management plans that benefit from collaborative team input. To help optimise patient care the meeting structure may change from time to time to give preference to areas that require more urgent attention or increased discussion time.
The meeting offers an excellent opportunity to hear and learn from a multitude of patient presentations, at times very complex clinical problems and the way the team addresses these. As a team member you will contribute your observations and knowledge about the clinical path of current inpatients.
Team members document treatment decisions made during the meeting for each inpatient. The responsible consultant or registrar might ask you to action items as required.